 |
Catastrophic Pressure Vessel
Failures: Learning from the Past |
ADAM HENSON, CHEMICAL SAFETY RECOMMENDATIONS SPECIALIST
U.S. CHEMICAL SAFETY AND HAZARD INVESTIGATION BOARD |
On April 8, 2021, at the Yenkin-Majestic Paint Corporation OPC Polymers Resin plant in Columbus, Ohio, the seal of a closed manway of a kettle failed, releasing a mixture of flammable naphtha solvent vapors. The vapors spread throughout the building and outside, igniting shortly thereafter.

The explosion at the Loy-Lange
Box Co. on April 3, 2017, resulted
in the death of one employee and
three workers at a nearby facility.
The explosion resulted in a fire that took over 100 firefighters almost 11 hours to extinguish. One employee was fatally crushed due to the building collapse. Eight other employees received injuries, including third-degree burns, fractures, and one requiring a leg amputation.
The U.S. Chemical Safety and Hazard Investigation Board (CSB) launched an investigation into the incident. The causes included the improper alteration of the kettle, ignoring a previous close call, and an overpressure event. This is not the first incident investigated by the CSB that is attributable to these causes.
The CSB
The CSB is a federal agency responsible for investigating accidental chemical releases. Following investigations, reports detailing the facts, conditions, and circumstances of these incidents are released to the public. In the CSB’s 25-plus-year history, nearly 200 catastrophic incidents have been investigated and 1,000 recommendations have been issued.
Several of those investigations focused on pressure vessel safety. These investigations include:
- D.D. Williamson & Co. Catastrophic Vessel Failure (DDW) (2003)
- Marcus Oil and Chemical Tank Explosion (MO&C) (2004)
- NDK Crystals Inc. Explosion with Offsite Fatality (NDK) (2009)
- Loy-Lange Box Company Pressure Vessel Explosion (Loy-Lange) (2017)
- Yenkin-Majestic Resin Plant Vapor Cloud Explosion and Fire (YM) (2021)
Here’s an explanation of the similarities among these incidents and key lessons for the industry.
Incident Descriptions
DDW: On April 11, 2003, a pressure vessel exploded at the D.D. Williamson Co., Inc. facility in Louisville. The explosion killed one employee and caused a release of 26,000 pounds of aqua ammonia, which resulted in a small evacuation in the community and a shelter-in-place order affecting 1,500 residents.
The incident occurred due to the vessel’s contents overheating, which led to overpressurization. The operators responsible for the process were conducting other duties leading up to the incident. The vessel had no overpressure protection, and previous damage to the vessel caused by the improper application of vacuum conditions is also believed to have contributed to the incident.

Loy-Lange officials did not adjust its operating practices after corrison was detected. More than half the records examined revealed an inadequate concentration of oxygen scavenger.
MO&C: On December 3, 2004, an explosion occurred at the Marcus Oil and Chemical facility in Houston, injuring several residents and three firefighters. Flying debris damaged the facility, nearby buildings, and vehicles within a quarter mile, and a 50,000-pound pressure vessel was displaced by approximately 150 feet.
The cause of the incident was the improper alteration of Tank 7. Marcus Oil cut an opening in Tanks 5-8 to install a steam pipe in each vessel. The process used to close these openings weakened the vessels. Also, on the day of the incident, compressed gas used to transfer product was supplied at a higher pressure than normal.
NDK: On December 7, 2009, a pressure vessel operating at 29,000 psig violently ruptured at the NDK Crystal, Inc. facility in Belvidere, Illinois. The vessel rupture caused pieces of structural steel to fly off the property, killing a truck driver at a gas station about 650 feet away. In addition, an adjacent automotive supply company was damaged, injuring one worker.

The cause of the Loy-Lange
incident was the improper repair
of the pressure vessel.
The cause of the incident was likely stress corrosion cracking (SCC). Microscopic examination of steel recovered from the incident revealed strong evidence of SCC. The vessels at NDK contained an alkaline sodium hydroxide and water solution generally known to damage some steels. An existing SCC surface-breaking fracture near the base of the vessel initiated the vessel rupture.
Loy-Lange: On April 3, 2017, a pressure vessel exploded at the Loy-Lange Box Co. facility in St. Louis. The explosion killed one employee and caused significant damage to the facility. The force of the explosion caused the vessel to fly off the property, killing three people at a neighboring facility.
The cause of the incident was the improper repair of the vessel. In 2012, a flush patch was installed to the bottom head of the vessel to repair damage caused by corrosion. During the repair, unacceptably thin material was left in place. Also, Loy-Lange’s operating practices were not sufficiently adjusted post-repair to prevent further corrosion.
NOTE: The Loy-Lange investigation was the BULLETIN cover story in the 2023 summer edition.
Similarities
In reviewing these incidents, themes become apparent. Recognition of these themes is important to facilitate incident prevention.
Improper R/A: A repair or alteration was made not in accordance with the National Board Inspection Code (NBIC) Part 3, Repairs and Alterations.
Forewarning: Defects in the vessels were known to the owner or user before the incident.
Overpressure: The process had insufficient controls to prevent overpressurization.
| |
Improper R/A |
Forewarning |
Overpressure |
| DDW |
|
|
X |
| MO&C |
X |
|
X |
| NDK |
|
X |
|
| Loy-Lange |
X |
X |
|
| YM |
X |
X |
X |
Improper R/A
As stated, the explosion at Yenkin-Majestic was caused by an improper alteration to Kettle 3. During an automation project, Kettle 3’s existing manway was permanently connected to a raw material feed hopper. Yenkin-Majestic hired a company to install a new manway so they could continue to access the inside of the vessel.
The original manway was rated to 50 psig. The new manway was intended to be rated for 16 psig. The fabricator cut a 20-inch hole in the top head of Kettle 3, welded on a nozzle, and attached a lid that closed onto a gasket to seal the assembly. There is no evidence that design calculations were performed to ensure the assembly could withstand 16 psig.
During the incident, the manway leak began at approximately 9 psig. Post-incident analysis of the new manway indicated a rating of 5 psig at best. The manway lid installed was 0.375 of an inch thick and secured with four bolts. To achieve the desired result of 16 psig, the manway would have needed a lid more than twice as thick and with twice as many bolts.
Similarly, the vessel involved in the MO&C incident was improperly altered. The closure weld used to reinstall the patch plate was fused less than 25% through and contained numerous flaws. The strength of the vessel in this area was reduced by more than 75%. The weld also created conditions likely to cause pressure-cycle-induced fatigue cracks.
The vessel involved in the Loy-Lange incident was also improperly repaired. Only a portion of the corroded pressure vessel bottom head was replaced. A thickness loss of as much as 95% was observed in the original material post-incident. On average, the original material left in place measured less than half the vessel’s design minimum thickness.
Forewarning
At Yenkin-Majestic, the altered vessel leaked from the gasket of the new manway the first time it was placed back into service. Instead of shutting down the equipment and investigating, Yenkin-Majestic changed the gasket to a thicker one and continued production. The kettle processed over 100 batches of resin before finally failing.
The safe operating condition of the vessel involved at NDK was questioned years before the incident. In January 2007, the closure head of another vessel in the facility experienced an uncontrolled leak.
NDK hired a consultant who determined that SCC caused the leak and that SCC was present in the facility’s other vessels. SCC was attributed to several issues. As a result of the consultant’s report, NDK’s insurer notified them that they reserved the right to deny claims related to these vessels.
Despite these warnings, NDK continued to operate its processes. The results of the 2007 investigation should have prompted further inspection of the vessels. SCC on the lid in 2007 was a clear indication that the vessels were not properly protected from this damage mechanism.
Finally, the defect in the vessel involved in the Loy-Lange incident was caused by oxygen pitting corrosion. Oxygen pitting corrosion is a widely known damage mechanism in steam generation systems. Preventing it requires removing dissolved oxygen from process water, which is generally accomplished by heating the water and adding chemicals.
In the days before the incident, water was observed leaking from the bottom of the vessel. Similar leaks were observed in this equipment in April 2004, August 2012, and November 2012. Additionally, at least two vendors notified Loy-Lange as early as 2004, and thereafter, that corrosion was pervasive throughout its steam generation system.
Despite recurring equipment failures due to corrosion and warnings from qualified vendors, Loy-Lange did not take action to ensure the mechanical integrity of its equipment. Loy-Lange also did not adjust its operating practices to prevent further corrosion. For example, over half of the records reviewed post-incident revealed an inadequate concentration of oxygen scavenger.
Overpressure
The overpressure event that led to the incident at Yenkin-Majestic resulted from adding flammable liquid solvent to the kettle while the agitator was not operating. The operator reset the agitator when he noticed it wasn’t operating. The activation of the agitator caused the solvent to mix with the hot resin and rapidly vaporize.
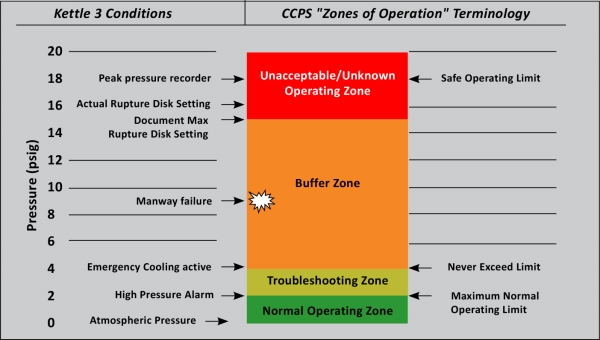
This figure is adapted from CCPS's "zones of operation" diagram to describe Kettle 3's operating parameters. Because of the improper alteration, the kettle failed prematurely in the "Buffer Zone" before the vessel's pressure safety device's set point.
The rapid vaporization of the solvent caused the pressure within the kettle to rise more than nine times than normal. The safeguards installed on the kettle were insufficient to respond to such a rapid increase in pressure. The gasket on the manway failed before the set pressure of the kettle’s rupture disk.

The explosion April 8, 2021, at
the Yenkin-Majestic Paint
Corporation OPC Polymers
Resin plant in Columbus, Ohio,
killed one person and injured
eight others.
The design of this process allowed operators to add solvent to the hot resin-filled kettle while the agitator was not operating. The process also did not prevent the agitator from starting up following the addition of the solvent. Yenkin-Majestic had not installed or configured interlocks to prevent these occurrences. The administrative controls Yenkin-Majestic relied upon were not effective in preventing the incident.
Similarly, the process involved in the incident at DDW was also not equipped with engineering controls to prevent the overpressurization of the vessel. This equipment was only equipped with a temperature gage and a pressure gage. The operators of this process were unaware that the vessel’s contents were overheating until they observed the product escaping. Moments later, the vessel exploded.
The vessel involved at MO&C was operating at a higher pressure than normal on the day of the incident. This was a conscious decision. The vessel was usually supplied with nitrogen at 45 psig, but on the day of the incident, it was supplied at 67 psig. This vessel had no automated process controls or engineering controls to address pressure.
Lessons for Industry
The consequences of improperly repairing or altering vessels, ignoring warning signs, and operating processes with insufficient controls can be disastrous.
To prevent future incidents:
- All repairs and alterations should be made in accordance with the requirements of NBIC Part 3. This is true regardless of whether a jurisdictional authority requires it and whether the owner or users believe it is necessary.
- Warning signs should be investigated to ensure the safe operation of equipment. Although NBIC Part 3 does not require an investigation of the conditions giving rise to a defect or an attempt to prevent future defects, these are necessary steps to ensure safety.
- Finally, processes relying heavily on human interaction will always be prone to failure. Owners or users should ensure that administrative controls alone are not relied upon to ensure safety. This is especially true for processes handling hazardous chemicals or operating at extreme pressure.
As the recurring themes in these incidents demonstrate, those who cannot remember the past are condemned to repeat it. For more information on these and other CSB investigations, go to csb.gov/investigations.